Coping With Pes Planus
Overview

The human foot is a complex structure that absorbs shock every time we take a step. The foot has to adapt to a variety of movements during different forms of activities such as walking, running and climbing steps. The foot is made up of many different joints, ligaments and muscles which have to work together to allow us to move and balance. The arch of the foot plays and important role in absorbing shock and preventing over stressing of the foot muscles and bones. In this article, we shall briefly discuss flat feet and fallen arches. These two conditions are closely related to each other and can increase the risk of overuse injury to the foot. They can also cause overload of more proximal structures such as ankles, shins, knees and the lower back.
Causes
Flat feet in adults can arise from a variety of causes. Here are the most common. An abnormality that is present from birth, stretched or torn tendons, damage or inflammation of the posterior tibial tendon (PTT), which connects from your lower leg, along your ankle, to the middle of the arch, broken or dislocated bones. Some health conditions, such as rheumatoid arthritis, Nerve problems. Other factors that can increase your risk include obesity, diabetes, ageing and Pregnancy.
Symptoms
Many people have flat feet and notice no problems and require no treatment. But others may experience the following symptoms, Feet tire easily, painful or achy feet, especially in the areas of the arches and heels, the inside bottom of your feet become swollen, foot movement, such as standing on your toes, is difficult, back and leg pain, If you notice any of these symptoms, it's time for a trip to the doctor.
Diagnosis
Your doctor examines your feet to determine two things, whether you have flat feet and the cause or causes. An exam may include the following steps, Checking your health history for evidence of illnesses or injuries that could be linked to flat feet or fallen arches, Looking at the soles of your shoes for unusual wear patterns, Observing the feet and legs as you stand and do simple movements, such as raising up on your toes, Testing the strength of muscles and tendons, including other tendons in the feet and legs, such as the Achilles tendon or the posterior tibial tendon, Taking X-rays or an MRI of your feet.
pes planus exercises
Non Surgical Treatment
If the condition is not bothering you or preventing you from being mobile, you may not need treatment (depending on your doctor?s diagnosis). Generally, treatment is reserved for those who have additional problems. Still, your doctor will probably recommend a simple treatment plan for your condition. This treatment may include rest and icing the arch, changing footwear, anti-inflammatory medication, using orthotics, over-the-counter medication such as ibuprofen, physical therapy. Corticosteroid injection (usually used in cases of severe pain). If these methods do not relieve symptoms of flat feet, your doctor may recommend surgery to reduce pain and improve the alignment of your bones.
Surgical Treatment
Feet that do not respond to the treatments above may need surgery. The surgery will help to create a supportive arch.
Prevention
Strap the arches into the anatomically correct positions with athletic tape and leave them like this for some time. If the fallen arches are an issue with the muscular structure, this may give the muscles an opportunity to strengthen. This is definitely not a fallen arches cure all the time but it can help prevent it more times than not. Ask a doctor or physical therapists to show you how to do this taping. Find shoes that fit. This may require that you get your foot measured and molded to ensure that the shoe will fit. Shoes that are too big, too tight or too short, may not directly cause the fallen arches, but they can assist with the damage to the area. These shoes should have thick cushioning inside and have plenty of room for your toes. Walk without shoes as much as possible. Shoes directly assist with weakening and distorting the arches of the feet so going without shoes can actually help strengthen your arches and prevent fallen arches. Walking on hard and bumpy surfaces barefooted makes the muscles in your feet strengthen in order to prevent injury. It is a coping mechanism by your body. Insert heel cups or insoles into the shoes that you wear the most. Many people wear uncomfortable shoes to work and these are the same shoes that cause their arches the most problems. Inserting the heel cups and insoles into these shoes can prevent fallen arches from occurring. Many people place these inserts into all their shoes to ensure support. Ask a medical professional, either your doctor or a physical therapist, about daily foot exercises that may keep the arches stronger than normal. Many times, you can find exercises and stretches on the Internet on various websites. Curling your toes tightly and rotating your feet will help strengthen your longitudinal arches. Relax your feet and shake them for a minute or so before you do any arch exercises. This will loosen the muscles in your feet that stay tight due to normal daily activities. Wear rigid soled sandals whenever possible to provide a strong support for your arches. Wooden soled sandals are the best ones if available. Walk or jog on concrete as much as you can. This will create a sturdy support for your arches. Running or walking in sandy areas or even on a treadmill, does not give rigid support. Instead, these surfaces absorb the step, offering no support for arches.
After Care
Patients may go home the day of surgery or they may require an overnight hospital stay. The leg will be placed in a splint or cast and should be kept elevated for the first two weeks. At that point, sutures are removed. A new cast or a removable boot is then placed. It is important that patients do not put any weight on the corrected foot for six to eight weeks following the operation. Patients may begin bearing weight at eight weeks and usually progress to full weightbearing by 10 to 12 weeks. For some patients, weightbearing requires additional time. After 12 weeks, patients commonly can transition to wearing a shoe. Inserts and ankle braces are often used. Physical therapy may be recommended. There are complications that relate to surgery in general. These include the risks associated with anesthesia, infection, damage to nerves and blood vessels, and bleeding or blood clots. Complications following flatfoot surgery may include wound breakdown or nonunion (incomplete healing of the bones). These complications often can be prevented with proper wound care and rehabilitation. Occasionally, patients may notice some discomfort due to prominent hardware. Removal of hardware can be done at a later time if this is an issue. The overall complication rates for flatfoot surgery are low.
The human foot is a complex structure that absorbs shock every time we take a step. The foot has to adapt to a variety of movements during different forms of activities such as walking, running and climbing steps. The foot is made up of many different joints, ligaments and muscles which have to work together to allow us to move and balance. The arch of the foot plays and important role in absorbing shock and preventing over stressing of the foot muscles and bones. In this article, we shall briefly discuss flat feet and fallen arches. These two conditions are closely related to each other and can increase the risk of overuse injury to the foot. They can also cause overload of more proximal structures such as ankles, shins, knees and the lower back.
Causes
Flat feet in adults can arise from a variety of causes. Here are the most common. An abnormality that is present from birth, stretched or torn tendons, damage or inflammation of the posterior tibial tendon (PTT), which connects from your lower leg, along your ankle, to the middle of the arch, broken or dislocated bones. Some health conditions, such as rheumatoid arthritis, Nerve problems. Other factors that can increase your risk include obesity, diabetes, ageing and Pregnancy.
Symptoms
Many people have flat feet and notice no problems and require no treatment. But others may experience the following symptoms, Feet tire easily, painful or achy feet, especially in the areas of the arches and heels, the inside bottom of your feet become swollen, foot movement, such as standing on your toes, is difficult, back and leg pain, If you notice any of these symptoms, it's time for a trip to the doctor.
Diagnosis
Your doctor examines your feet to determine two things, whether you have flat feet and the cause or causes. An exam may include the following steps, Checking your health history for evidence of illnesses or injuries that could be linked to flat feet or fallen arches, Looking at the soles of your shoes for unusual wear patterns, Observing the feet and legs as you stand and do simple movements, such as raising up on your toes, Testing the strength of muscles and tendons, including other tendons in the feet and legs, such as the Achilles tendon or the posterior tibial tendon, Taking X-rays or an MRI of your feet.
pes planus exercises
Non Surgical Treatment
If the condition is not bothering you or preventing you from being mobile, you may not need treatment (depending on your doctor?s diagnosis). Generally, treatment is reserved for those who have additional problems. Still, your doctor will probably recommend a simple treatment plan for your condition. This treatment may include rest and icing the arch, changing footwear, anti-inflammatory medication, using orthotics, over-the-counter medication such as ibuprofen, physical therapy. Corticosteroid injection (usually used in cases of severe pain). If these methods do not relieve symptoms of flat feet, your doctor may recommend surgery to reduce pain and improve the alignment of your bones.
Surgical Treatment
Feet that do not respond to the treatments above may need surgery. The surgery will help to create a supportive arch.
Prevention
Strap the arches into the anatomically correct positions with athletic tape and leave them like this for some time. If the fallen arches are an issue with the muscular structure, this may give the muscles an opportunity to strengthen. This is definitely not a fallen arches cure all the time but it can help prevent it more times than not. Ask a doctor or physical therapists to show you how to do this taping. Find shoes that fit. This may require that you get your foot measured and molded to ensure that the shoe will fit. Shoes that are too big, too tight or too short, may not directly cause the fallen arches, but they can assist with the damage to the area. These shoes should have thick cushioning inside and have plenty of room for your toes. Walk without shoes as much as possible. Shoes directly assist with weakening and distorting the arches of the feet so going without shoes can actually help strengthen your arches and prevent fallen arches. Walking on hard and bumpy surfaces barefooted makes the muscles in your feet strengthen in order to prevent injury. It is a coping mechanism by your body. Insert heel cups or insoles into the shoes that you wear the most. Many people wear uncomfortable shoes to work and these are the same shoes that cause their arches the most problems. Inserting the heel cups and insoles into these shoes can prevent fallen arches from occurring. Many people place these inserts into all their shoes to ensure support. Ask a medical professional, either your doctor or a physical therapist, about daily foot exercises that may keep the arches stronger than normal. Many times, you can find exercises and stretches on the Internet on various websites. Curling your toes tightly and rotating your feet will help strengthen your longitudinal arches. Relax your feet and shake them for a minute or so before you do any arch exercises. This will loosen the muscles in your feet that stay tight due to normal daily activities. Wear rigid soled sandals whenever possible to provide a strong support for your arches. Wooden soled sandals are the best ones if available. Walk or jog on concrete as much as you can. This will create a sturdy support for your arches. Running or walking in sandy areas or even on a treadmill, does not give rigid support. Instead, these surfaces absorb the step, offering no support for arches.
After Care
Patients may go home the day of surgery or they may require an overnight hospital stay. The leg will be placed in a splint or cast and should be kept elevated for the first two weeks. At that point, sutures are removed. A new cast or a removable boot is then placed. It is important that patients do not put any weight on the corrected foot for six to eight weeks following the operation. Patients may begin bearing weight at eight weeks and usually progress to full weightbearing by 10 to 12 weeks. For some patients, weightbearing requires additional time. After 12 weeks, patients commonly can transition to wearing a shoe. Inserts and ankle braces are often used. Physical therapy may be recommended. There are complications that relate to surgery in general. These include the risks associated with anesthesia, infection, damage to nerves and blood vessels, and bleeding or blood clots. Complications following flatfoot surgery may include wound breakdown or nonunion (incomplete healing of the bones). These complications often can be prevented with proper wound care and rehabilitation. Occasionally, patients may notice some discomfort due to prominent hardware. Removal of hardware can be done at a later time if this is an issue. The overall complication rates for flatfoot surgery are low.
Heel Painfulness All You Ought To Understand Heel Serious Pain
Overview
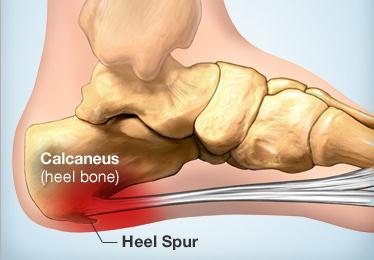
Heel pain can vary from moderate to severe pain that can make walking and daily tasks a chore if not treated. There are a number of different conditions which can cause heel pain so it is important that your heel is properly assessed and diagnosed by a Podiatrist. The most common cause of heel pain is plantar fasciitis. This is where the tissue becomes inflamed at the heel bone or along sole of the foot between the heel and toe. Another condition commonly referred to as a heel spur can also cause pain in the heel. A heel spur is when a spike of bone has been pulled away from the heel bone, where the plantar fascia inserts, causing pain in the area directly under the heel on direct pressure.
Causes
Heel pain is a common symptom that has many possible causes. Although heel pain sometimes is caused by a systemic (body-wide) illness, such as rheumatoid arthritis or gout, it usually is a local condition that affects only the foot. The most common local causes of heel pain include Plantar fasciitis. lantar fasciitis is a painful inflammation of the plantar fascia, a fibrous band of tissue on the sole of the foot that helps to support the arch. Plantar fasciitis occurs when the plantar fascia is overloaded or overstretched. This causes small tears in the fibers of the fascia, especially where the fascia meets the heel bone. Plantar fasciitis may develop in just about anyone but it is particularly common in the following groups of people: people with diabetes, obese people, pregnant women, runners, volleyball players, tennis players and people who participate in step aerobics or stair climbing. You also can trigger plantar fasciitis by pushing a large appliance or piece of furniture or by wearing worn out or poorly constructed shoes. In athletes, plantar fasciitis may follow a period of intense training, especially in runners who push themselves to run longer distances. People with flat feet have a higher risk of developing plantar fasciitis. Heel spur. heel spur is an abnormal growth of bone at the area where the plantar fascia attaches to the heel bone. It is caused by long-term strain on the plantar fascia and muscles of the foot, especially in obese people, runners or joggers. As in plantar fasciitis, shoes that are worn out, poorly fitting or poorly constructed can aggravate the problem. Heel spurs may not be the cause of heel pain even when seen on an X-ray. In fact, they may develop as a reaction to plantar fasciitis. Calcaneal apophysitis, n this condition, the center of the heel bone becomes irritated as a result of a new shoe or increased athletic activity. This pain occurs in the back of the heel, not the bottom. Calcaneal apophysitis is a fairly common cause of heel pain in active, growing children between the ages of 8 and 14. Although almost any boy or girl can be affected, children who participate in sports that require a lot of jumping have the highest risk of developing this condition. Bursitis. ursitis means inflammation of a bursa, a sac that lines many joints and allows tendons and muscles to move easily when the joint is moving. In the heel, bursitis may cause pain at the underside or back of the heel. In some cases, heel bursitis is related to structural problems of the foot that cause an abnormal gait (way of walking). In other cases, wearing shoes with poorly cushioned heels can trigger bursitis. Pump bump. his condition, medically known as posterior calcaneal exostosis, is an abnormal bony growth at the back of the heel. It is especially common in young women, in whom it is often related to long-term bursitis caused by pressure from pump shoes. Local bruises. ike other parts of the foot, the heel can be bumped and bruised accidentally. Typically, this happens as a "stone bruise," an impact injury caused by stepping on a sharp object while walking barefoot. Achilles tendonitis. n most cases, Achilles tendonitis (inflammation of the Achilles tendon) is triggered by overuse, especially by excessive jumping during sports. However, it also can be related to poorly fitting shoes if the upper back portion of a shoe digs into the Achilles tendon at the back of the heel. Less often, it is caused by an inflammatory illness, such as ankylosing spondylitis (also called axial spondylarthritis), reactive arthritis, gout or rheumatoid arthritis. Trapped nerve. ompression of a small nerve (a branch of the lateral plantar nerve) can cause pain, numbness or tingling in the heel area. In many cases, this nerve compression is related to a sprain, fracture or varicose (swollen) vein near the heel.
Symptoms
Pain typically comes on gradually, with no injury to the affected area. It is frequently triggered by wearing a flat shoe, such as flip-flop sandals. Flat footwear may stretch the plantar fascia to such an extent that the area becomes swollen (inflamed). In most cases, the pain is under the foot, toward the front of the heel. Post-static dyskinesia (pain after rest) symptoms tend to be worse just after getting out of bed in the morning, and after a period of rest during the day. After a bit of activity symptoms often improve a bit. However, they may worsen again toward the end of the day.
Diagnosis
Depending on the condition, the cause of heel pain is diagnosed using a number of tests, including medical history, physical examination, including examination of joints and muscles of the foot and leg, X-rays.
Non Surgical Treatment
Treatments to add to your stretching program include wearing good-quality shoes, icing the painful area, and massaging the arch. Do not walk barefoot; walk in shoes with good heel and arch supports such as high-quality walking or running shoes. Keep a pair of shoes next to your bed so you can put them on before taking your first step. Your doctor may recommend that you wear an additional arch support or a heel cup in the shoes. Icing your foot can help relieve pain. Rub a frozen bottle of water or an ice cup over the tender areas for five minutes two times each day. Massage your foot by rolling a tennis, golf ball, or baseball along your sole and heel. This friction massage can help break up adhesions and stretch the plantar fascia. Do this for five minutes two times each day. If you are a runner or just started a walking or running program, evaluate your training for errors such as warming up improperly, increasing mileage too quickly, running hills excessively, running on surfaces that are too hard, or wearing broken down shoes. Adjusting your training program can help relieve your pain. While recovering from heel pain, walk or jog in a pool or crosstrain by biking and swimming. These activities maintain your cardiovascular fitness without stressing your heel cord or plantar fascia. Heel pain takes time to go away. Be patient and remember that no treatment is a substitute for STRETCHING!
Surgical Treatment
At most 95% of heel pain can be treated without surgery. A very low percentage of people really need to have surgery on the heel. It is a biomechanical problem and it?s very imperative that you not only get evaluated, but receive care immediately. Having heel pain is like having a problem with your eyes; as you would get glasses to correct your eyes, you should look into orthotics to correct your foot. Orthotics are sort of like glasses for the feet. They correct and realign the foot to put them into neutral or normal position to really prevent heel pain, and many other foot issues. Whether it be bunions, hammertoes, neuromas, or even ankle instability, a custom orthotic is something worth considering.
heel cups for achilles tendonitis
Prevention

Maintaining flexible and strong muscles in your calves, ankles, and feet can help prevent some types of heel pain. Always stretch and warm-up before exercising. Wear comfortable, properly fitting shoes with good arch support and cushioning. Make sure there is enough room for your toes.
Heel pain can vary from moderate to severe pain that can make walking and daily tasks a chore if not treated. There are a number of different conditions which can cause heel pain so it is important that your heel is properly assessed and diagnosed by a Podiatrist. The most common cause of heel pain is plantar fasciitis. This is where the tissue becomes inflamed at the heel bone or along sole of the foot between the heel and toe. Another condition commonly referred to as a heel spur can also cause pain in the heel. A heel spur is when a spike of bone has been pulled away from the heel bone, where the plantar fascia inserts, causing pain in the area directly under the heel on direct pressure.
Causes
Heel pain is a common symptom that has many possible causes. Although heel pain sometimes is caused by a systemic (body-wide) illness, such as rheumatoid arthritis or gout, it usually is a local condition that affects only the foot. The most common local causes of heel pain include Plantar fasciitis. lantar fasciitis is a painful inflammation of the plantar fascia, a fibrous band of tissue on the sole of the foot that helps to support the arch. Plantar fasciitis occurs when the plantar fascia is overloaded or overstretched. This causes small tears in the fibers of the fascia, especially where the fascia meets the heel bone. Plantar fasciitis may develop in just about anyone but it is particularly common in the following groups of people: people with diabetes, obese people, pregnant women, runners, volleyball players, tennis players and people who participate in step aerobics or stair climbing. You also can trigger plantar fasciitis by pushing a large appliance or piece of furniture or by wearing worn out or poorly constructed shoes. In athletes, plantar fasciitis may follow a period of intense training, especially in runners who push themselves to run longer distances. People with flat feet have a higher risk of developing plantar fasciitis. Heel spur. heel spur is an abnormal growth of bone at the area where the plantar fascia attaches to the heel bone. It is caused by long-term strain on the plantar fascia and muscles of the foot, especially in obese people, runners or joggers. As in plantar fasciitis, shoes that are worn out, poorly fitting or poorly constructed can aggravate the problem. Heel spurs may not be the cause of heel pain even when seen on an X-ray. In fact, they may develop as a reaction to plantar fasciitis. Calcaneal apophysitis, n this condition, the center of the heel bone becomes irritated as a result of a new shoe or increased athletic activity. This pain occurs in the back of the heel, not the bottom. Calcaneal apophysitis is a fairly common cause of heel pain in active, growing children between the ages of 8 and 14. Although almost any boy or girl can be affected, children who participate in sports that require a lot of jumping have the highest risk of developing this condition. Bursitis. ursitis means inflammation of a bursa, a sac that lines many joints and allows tendons and muscles to move easily when the joint is moving. In the heel, bursitis may cause pain at the underside or back of the heel. In some cases, heel bursitis is related to structural problems of the foot that cause an abnormal gait (way of walking). In other cases, wearing shoes with poorly cushioned heels can trigger bursitis. Pump bump. his condition, medically known as posterior calcaneal exostosis, is an abnormal bony growth at the back of the heel. It is especially common in young women, in whom it is often related to long-term bursitis caused by pressure from pump shoes. Local bruises. ike other parts of the foot, the heel can be bumped and bruised accidentally. Typically, this happens as a "stone bruise," an impact injury caused by stepping on a sharp object while walking barefoot. Achilles tendonitis. n most cases, Achilles tendonitis (inflammation of the Achilles tendon) is triggered by overuse, especially by excessive jumping during sports. However, it also can be related to poorly fitting shoes if the upper back portion of a shoe digs into the Achilles tendon at the back of the heel. Less often, it is caused by an inflammatory illness, such as ankylosing spondylitis (also called axial spondylarthritis), reactive arthritis, gout or rheumatoid arthritis. Trapped nerve. ompression of a small nerve (a branch of the lateral plantar nerve) can cause pain, numbness or tingling in the heel area. In many cases, this nerve compression is related to a sprain, fracture or varicose (swollen) vein near the heel.
Symptoms
Pain typically comes on gradually, with no injury to the affected area. It is frequently triggered by wearing a flat shoe, such as flip-flop sandals. Flat footwear may stretch the plantar fascia to such an extent that the area becomes swollen (inflamed). In most cases, the pain is under the foot, toward the front of the heel. Post-static dyskinesia (pain after rest) symptoms tend to be worse just after getting out of bed in the morning, and after a period of rest during the day. After a bit of activity symptoms often improve a bit. However, they may worsen again toward the end of the day.
Diagnosis
Depending on the condition, the cause of heel pain is diagnosed using a number of tests, including medical history, physical examination, including examination of joints and muscles of the foot and leg, X-rays.
Non Surgical Treatment
Treatments to add to your stretching program include wearing good-quality shoes, icing the painful area, and massaging the arch. Do not walk barefoot; walk in shoes with good heel and arch supports such as high-quality walking or running shoes. Keep a pair of shoes next to your bed so you can put them on before taking your first step. Your doctor may recommend that you wear an additional arch support or a heel cup in the shoes. Icing your foot can help relieve pain. Rub a frozen bottle of water or an ice cup over the tender areas for five minutes two times each day. Massage your foot by rolling a tennis, golf ball, or baseball along your sole and heel. This friction massage can help break up adhesions and stretch the plantar fascia. Do this for five minutes two times each day. If you are a runner or just started a walking or running program, evaluate your training for errors such as warming up improperly, increasing mileage too quickly, running hills excessively, running on surfaces that are too hard, or wearing broken down shoes. Adjusting your training program can help relieve your pain. While recovering from heel pain, walk or jog in a pool or crosstrain by biking and swimming. These activities maintain your cardiovascular fitness without stressing your heel cord or plantar fascia. Heel pain takes time to go away. Be patient and remember that no treatment is a substitute for STRETCHING!
Surgical Treatment
At most 95% of heel pain can be treated without surgery. A very low percentage of people really need to have surgery on the heel. It is a biomechanical problem and it?s very imperative that you not only get evaluated, but receive care immediately. Having heel pain is like having a problem with your eyes; as you would get glasses to correct your eyes, you should look into orthotics to correct your foot. Orthotics are sort of like glasses for the feet. They correct and realign the foot to put them into neutral or normal position to really prevent heel pain, and many other foot issues. Whether it be bunions, hammertoes, neuromas, or even ankle instability, a custom orthotic is something worth considering.
heel cups for achilles tendonitis
Prevention
Maintaining flexible and strong muscles in your calves, ankles, and feet can help prevent some types of heel pain. Always stretch and warm-up before exercising. Wear comfortable, properly fitting shoes with good arch support and cushioning. Make sure there is enough room for your toes.
Leg Length Discrepancy Following Hip Replacement
Overview
A Leg Length Inequality or Leg Length Discrepancy is exactly as it sounds. One or more bones (the Femur or thigh bone, the Tibia or shin bone, and/or the joint spacing within the knee) are unequal in total length when measured in comparison to the same structures on the opposite side. It is common for people to have one leg longer than the other. In fact, it is more typical to be asymmetrical than it is to be symmetrical.
Causes
The causes of LLD may be divided into those that shorten a limb versus those that lengthen a limb, or they may be classified as affecting the length versus the rate of growth in a limb. For example, a fracture that heals poorly may shorten a leg slightly, but does not affect its growth rate. Radiation, on the other hand, can affect a leg's long-term ability to expand, but does not acutely affect its length. Causes that shorten the leg are more common than those that lengthen it and include congenital growth deficiencies (seen in hemiatrophy and skeletal dysplasias ), infections that infiltrate the epiphysis (e.g. osteomyelitis ), tumors, fractures that occur through the growth plate or have overriding ends, Legg-Calve-Perthes disease, slipped capital femoral epiphysis (SCFE), and radiation. Lengthening can result from unique conditions, such as hemihypertrophy , in which one or more structures on one side of the body become larger than the other side, vascular malformations or tumors (such as hemangioma ), which cause blood flow on one side to exceed that of the other, Wilm's tumor (of the kidney), septic arthritis, healed fractures, or orthopaedic surgery. Leg length discrepancy may arise from a problem in almost any portion of the femur or tibia. For example, fractures can occur at virtually all levels of the two bones. Fractures or other problems of the fibula do not lead to LLD, as long as the more central, weight-bearing tibia is unaffected. Because many cases of LLD are due to decreased rate of growth, the femoral or tibial epiphyses are commonly affected regions.
Symptoms
The patient/athlete may present with an altered gait (such as limping) and/or scoliosis and/or low back pain. Lower extremity disorders are possibly associated with LLD, some of these are increased hip pain and degeneration (especially involving the long leg). Increased risk of: knee injury, ITB syndrome, pronation and plantar fascitis, asymmetrical strength in lower extremity. Increased disc or vertebral degeneration. Symptoms vary between patients, some patients may complain of just headaches.
Diagnosis
A qualified musculoskeletal expert will first take a medical history and conduct a physical exam. Other tests may include X-rays, MRI, or CT scan to diagnose the root cause.
Non Surgical Treatment
The most common solution to rectify the difference in your leg lengths is to compensate for the short fall in your shortest leg, thereby making both of your legs structurally the same length. Surgery is a drastic option and extremely rare, mainly because the results are not guaranteed aswell as the risks associated with surgery, not to mention the inconvenience of waiting until your broken bones are healed. Instead, orthopediatrician's will almost always advise on the use of "heel lifts for leg length discrepancy". These are a quick, simple and costs effective solution. They sit under your heel, inside your shoe and elevate your shorter leg by the same amount as the discrepancy. Most heel lifts are adjustable and come in a range of sizes. Such lifts can instantly correct a leg length discrepancy and prevent the cause of associate risks.

leg length discrepancy test
Surgical Treatment
Surgeries for LLD are designed to do one of three general things ? shorten the long leg, stop or slow the growth of the longer or more rapidly growing leg, or lengthen the short leg. Stopping the growth of the longer leg is the most commonly utilized of the three approaches and involves an operation known as an epiphysiodesis , in which the growth plate of either the lower femur or upper tibia is visualized in the operating room using fluoroscopy (a type of real-time radiographic imaging) and ablated , which involves drilling into the region several times, such that the tissue is no longer capable of bone growth. Because the epiphyseal growth capabilities cannot be restored following the surgery, proper timing is crucial. Usually the operation is planned for the last 2 to 3 years of growth and has excellent results, with children leaving the hospital within a few days with good mobility. However, it is only appropriate for LLD of under 5cm.
A Leg Length Inequality or Leg Length Discrepancy is exactly as it sounds. One or more bones (the Femur or thigh bone, the Tibia or shin bone, and/or the joint spacing within the knee) are unequal in total length when measured in comparison to the same structures on the opposite side. It is common for people to have one leg longer than the other. In fact, it is more typical to be asymmetrical than it is to be symmetrical.
Causes
The causes of LLD may be divided into those that shorten a limb versus those that lengthen a limb, or they may be classified as affecting the length versus the rate of growth in a limb. For example, a fracture that heals poorly may shorten a leg slightly, but does not affect its growth rate. Radiation, on the other hand, can affect a leg's long-term ability to expand, but does not acutely affect its length. Causes that shorten the leg are more common than those that lengthen it and include congenital growth deficiencies (seen in hemiatrophy and skeletal dysplasias ), infections that infiltrate the epiphysis (e.g. osteomyelitis ), tumors, fractures that occur through the growth plate or have overriding ends, Legg-Calve-Perthes disease, slipped capital femoral epiphysis (SCFE), and radiation. Lengthening can result from unique conditions, such as hemihypertrophy , in which one or more structures on one side of the body become larger than the other side, vascular malformations or tumors (such as hemangioma ), which cause blood flow on one side to exceed that of the other, Wilm's tumor (of the kidney), septic arthritis, healed fractures, or orthopaedic surgery. Leg length discrepancy may arise from a problem in almost any portion of the femur or tibia. For example, fractures can occur at virtually all levels of the two bones. Fractures or other problems of the fibula do not lead to LLD, as long as the more central, weight-bearing tibia is unaffected. Because many cases of LLD are due to decreased rate of growth, the femoral or tibial epiphyses are commonly affected regions.
Symptoms
The patient/athlete may present with an altered gait (such as limping) and/or scoliosis and/or low back pain. Lower extremity disorders are possibly associated with LLD, some of these are increased hip pain and degeneration (especially involving the long leg). Increased risk of: knee injury, ITB syndrome, pronation and plantar fascitis, asymmetrical strength in lower extremity. Increased disc or vertebral degeneration. Symptoms vary between patients, some patients may complain of just headaches.
Diagnosis
A qualified musculoskeletal expert will first take a medical history and conduct a physical exam. Other tests may include X-rays, MRI, or CT scan to diagnose the root cause.
Non Surgical Treatment
The most common solution to rectify the difference in your leg lengths is to compensate for the short fall in your shortest leg, thereby making both of your legs structurally the same length. Surgery is a drastic option and extremely rare, mainly because the results are not guaranteed aswell as the risks associated with surgery, not to mention the inconvenience of waiting until your broken bones are healed. Instead, orthopediatrician's will almost always advise on the use of "heel lifts for leg length discrepancy". These are a quick, simple and costs effective solution. They sit under your heel, inside your shoe and elevate your shorter leg by the same amount as the discrepancy. Most heel lifts are adjustable and come in a range of sizes. Such lifts can instantly correct a leg length discrepancy and prevent the cause of associate risks.
leg length discrepancy test
Surgical Treatment
Surgeries for LLD are designed to do one of three general things ? shorten the long leg, stop or slow the growth of the longer or more rapidly growing leg, or lengthen the short leg. Stopping the growth of the longer leg is the most commonly utilized of the three approaches and involves an operation known as an epiphysiodesis , in which the growth plate of either the lower femur or upper tibia is visualized in the operating room using fluoroscopy (a type of real-time radiographic imaging) and ablated , which involves drilling into the region several times, such that the tissue is no longer capable of bone growth. Because the epiphyseal growth capabilities cannot be restored following the surgery, proper timing is crucial. Usually the operation is planned for the last 2 to 3 years of growth and has excellent results, with children leaving the hospital within a few days with good mobility. However, it is only appropriate for LLD of under 5cm.
Leg Length Discrepancy The Galeazzi Test
Overview
The majority of people in the world actually have some degree of leg length discrepancy, up to 2cm. One study found that only around 1/4 of people have legs of equal lengths. LLD of greater than 2cm is relatively rare, however, and the greater the discrepancy, the greater the chances of having a clinical problem down the road. A limp generally begins when LLD exceeds 2cm and becomes extremely noticeable above 3cm. When patients with LLD develop an abnormal gait, one of the debilitating clinical features can be fatigue because of the relatively high amount of energy needed to walk in the new, inefficient way. Poliomyelitis, or polio, as it is more commonly known, used to account for around 1/3 of all cases of LLD, but due to the effectiveness of polio vaccines, it now represents a negligible cause of the condition. Functional LLD, described above, usually involves treatment focused on the hip, pelvis, and/or lower back, rather than the leg. If you have been diagnosed with functional LLD or pelvic obliquity, please ask your orthopaedic surgeon for more information about treatment of these conditions.
Causes
LLDs are very common. Sometimes the cause isn?t known. But the known causes of LLD in children include, injury or infection that slows growth of one leg bone. Injury to the growth plate (a soft part of a long bone that allows the bone to grow). Growth plate injury can slow bone growth in that leg. Fracture to a leg bone that causes overgrowth of the bone as it heals. A congenital (present at birth) problem (one whole side of the child?s body may be larger than the other side). Conditions that affect muscles and nerves, such as polio.
Symptoms
Faulty feet and ankle structure profoundly affect leg length and pelvic positioning. The most common asymmetrical foot position is the pronated foot. Sensory receptors embedded on the bottom of the foot alert the brain to the slightest weight shift. Since the brain is always trying to maintain pelvic balance, when presented with a long left leg, it attempts to adapt to the altered weight shift by dropping the left medial arch (shortening the long leg) and supinating the right arch to lengthen the short leg.1 Left unchecked, excessive foot pronation will internally rotate the left lower extremity, causing excessive strain to the lateral meniscus and medial collateral knee ligaments. Conversely, excessive supination tends to externally rotate the leg and thigh, creating opposite knee, hip and pelvic distortions.
Diagnosis
The only way to decipher between anatomical and functional leg length inequalities (you can have both) is by a physical measurement and series of biomechanical tests. It is actually a simple process and gets to the true cause of some runner?s chronic foot, knee, hip and back pain. After the muscles are tested and the legs are measured it may be necessary to get a special X-ray that measures both of your thighs (Femurs) and legs (Tibias). The X-ray is read by a medical radiologist who provides a report of the actual difference down to the micrometer leaving zero room for error. Once the difference in leg length is known, the solution becomes clear.
Non Surgical Treatment
The treatment of LLD depends primarily on the diagnosed cause, the age of the patient, and the severity of the discrepancy. Non-operative treatment is usually the first step in management and, in many cases, LLD is mild or is predicted to lessen in the future, based on growth rate estimates in the two legs. In such cases, no treatment may be necessary or can be delayed until a later stage of physical maturity that allows for clearer prognostic approximation. For LLD of 2cm to 2.5cm, treatment may be as simple as insertion of a heel lift or other shoe insert that evens out leg lengths, so to speak. For more severe cases, heel lifts can affect patient comfort when walking, decrease ankle stability, and greatly increase the risk of sprains. For infants with congenital shortening of the limb, a prosthetic ? often a custom-fit splint made of polypropylene ? may be successful in treating more severe LLD without surgery. In many instances, however, a surgical operation is the best treatment for LLD.

leg length discrepancy test
Surgical Treatment
Surgical operations to equalize leg lengths include the following. Shortening the longer leg. This is usually done if growth is already complete, and the patient is tall enough that losing an inch is not a problem. Slowing or stopping the growth of the longer leg. Growth of the lower limbs take place mainly in the epiphyseal plates (growth plates) of the lower femur and upper tibia and fibula. Stapling the growth plates in a child for a few years theoretically will stop growth for the period, and when the staples were removed, growth was supposed to resume. This procedure was quite popular till it was found that the amount of growth retarded was not certain, and when the staples where removed, the bone failed to resume its growth. Hence epiphyseal stapling has now been abandoned for the more reliable Epiphyseodesis. By use of modern fluoroscopic equipment, the surgeon can visualize the growth plate, and by making small incisions and using multiple drillings, the growth plate of the lower femur and/or upper tibia and fibula can be ablated. Since growth is stopped permanently by this procedure, the timing of the operation is crucial. This is probably the most commonly done procedure for correcting leg length discrepancy. But there is one limitation. The maximum amount of discrepancy that can be corrected by Epiphyseodesis is 5 cm. Lengthening the short leg. Various procedures have been done over the years to effect this result. External fixation devices are usually needed to hold the bone that is being lengthened. In the past, the bone to be lengthened was cut, and using the external fixation device, the leg was stretched out gradually over weeks. A gap in the bone was thus created, and a second operation was needed to place a bone block in the gap for stability and induce healing as a graft. More recently, a new technique called callotasis is being use. The bone to be lengthened is not cut completely, only partially and called a corticotomy. The bone is then distracted over an external device (usually an Ilizarov or Orthofix apparatus) very slowly so that bone healing is proceeding as the lengthening is being done. This avoids the need for a second procedure to insert bone graft. The procedure involved in leg lengthening is complicated, and fraught with risks. Theoretically, there is no limit to how much lengthening one can obtain, although the more ambitious one is, the higher the complication rate.
The majority of people in the world actually have some degree of leg length discrepancy, up to 2cm. One study found that only around 1/4 of people have legs of equal lengths. LLD of greater than 2cm is relatively rare, however, and the greater the discrepancy, the greater the chances of having a clinical problem down the road. A limp generally begins when LLD exceeds 2cm and becomes extremely noticeable above 3cm. When patients with LLD develop an abnormal gait, one of the debilitating clinical features can be fatigue because of the relatively high amount of energy needed to walk in the new, inefficient way. Poliomyelitis, or polio, as it is more commonly known, used to account for around 1/3 of all cases of LLD, but due to the effectiveness of polio vaccines, it now represents a negligible cause of the condition. Functional LLD, described above, usually involves treatment focused on the hip, pelvis, and/or lower back, rather than the leg. If you have been diagnosed with functional LLD or pelvic obliquity, please ask your orthopaedic surgeon for more information about treatment of these conditions.
Causes
LLDs are very common. Sometimes the cause isn?t known. But the known causes of LLD in children include, injury or infection that slows growth of one leg bone. Injury to the growth plate (a soft part of a long bone that allows the bone to grow). Growth plate injury can slow bone growth in that leg. Fracture to a leg bone that causes overgrowth of the bone as it heals. A congenital (present at birth) problem (one whole side of the child?s body may be larger than the other side). Conditions that affect muscles and nerves, such as polio.
Symptoms
Faulty feet and ankle structure profoundly affect leg length and pelvic positioning. The most common asymmetrical foot position is the pronated foot. Sensory receptors embedded on the bottom of the foot alert the brain to the slightest weight shift. Since the brain is always trying to maintain pelvic balance, when presented with a long left leg, it attempts to adapt to the altered weight shift by dropping the left medial arch (shortening the long leg) and supinating the right arch to lengthen the short leg.1 Left unchecked, excessive foot pronation will internally rotate the left lower extremity, causing excessive strain to the lateral meniscus and medial collateral knee ligaments. Conversely, excessive supination tends to externally rotate the leg and thigh, creating opposite knee, hip and pelvic distortions.
Diagnosis
The only way to decipher between anatomical and functional leg length inequalities (you can have both) is by a physical measurement and series of biomechanical tests. It is actually a simple process and gets to the true cause of some runner?s chronic foot, knee, hip and back pain. After the muscles are tested and the legs are measured it may be necessary to get a special X-ray that measures both of your thighs (Femurs) and legs (Tibias). The X-ray is read by a medical radiologist who provides a report of the actual difference down to the micrometer leaving zero room for error. Once the difference in leg length is known, the solution becomes clear.
Non Surgical Treatment
The treatment of LLD depends primarily on the diagnosed cause, the age of the patient, and the severity of the discrepancy. Non-operative treatment is usually the first step in management and, in many cases, LLD is mild or is predicted to lessen in the future, based on growth rate estimates in the two legs. In such cases, no treatment may be necessary or can be delayed until a later stage of physical maturity that allows for clearer prognostic approximation. For LLD of 2cm to 2.5cm, treatment may be as simple as insertion of a heel lift or other shoe insert that evens out leg lengths, so to speak. For more severe cases, heel lifts can affect patient comfort when walking, decrease ankle stability, and greatly increase the risk of sprains. For infants with congenital shortening of the limb, a prosthetic ? often a custom-fit splint made of polypropylene ? may be successful in treating more severe LLD without surgery. In many instances, however, a surgical operation is the best treatment for LLD.
leg length discrepancy test
Surgical Treatment
Surgical operations to equalize leg lengths include the following. Shortening the longer leg. This is usually done if growth is already complete, and the patient is tall enough that losing an inch is not a problem. Slowing or stopping the growth of the longer leg. Growth of the lower limbs take place mainly in the epiphyseal plates (growth plates) of the lower femur and upper tibia and fibula. Stapling the growth plates in a child for a few years theoretically will stop growth for the period, and when the staples were removed, growth was supposed to resume. This procedure was quite popular till it was found that the amount of growth retarded was not certain, and when the staples where removed, the bone failed to resume its growth. Hence epiphyseal stapling has now been abandoned for the more reliable Epiphyseodesis. By use of modern fluoroscopic equipment, the surgeon can visualize the growth plate, and by making small incisions and using multiple drillings, the growth plate of the lower femur and/or upper tibia and fibula can be ablated. Since growth is stopped permanently by this procedure, the timing of the operation is crucial. This is probably the most commonly done procedure for correcting leg length discrepancy. But there is one limitation. The maximum amount of discrepancy that can be corrected by Epiphyseodesis is 5 cm. Lengthening the short leg. Various procedures have been done over the years to effect this result. External fixation devices are usually needed to hold the bone that is being lengthened. In the past, the bone to be lengthened was cut, and using the external fixation device, the leg was stretched out gradually over weeks. A gap in the bone was thus created, and a second operation was needed to place a bone block in the gap for stability and induce healing as a graft. More recently, a new technique called callotasis is being use. The bone to be lengthened is not cut completely, only partially and called a corticotomy. The bone is then distracted over an external device (usually an Ilizarov or Orthofix apparatus) very slowly so that bone healing is proceeding as the lengthening is being done. This avoids the need for a second procedure to insert bone graft. The procedure involved in leg lengthening is complicated, and fraught with risks. Theoretically, there is no limit to how much lengthening one can obtain, although the more ambitious one is, the higher the complication rate.
Working with Mortons Neuroma
Overview
 Morton neuroma (interdigital neuroma), first described in 1876, is a perineural fibrosis and nerve degeneration of the common digital nerve. Morton neuroma, or Morton's neuroma, is not a true neuroma, although it results in neuropathic pain in the distribution of the interdigital nerve secondary to repetitive irritation of the nerve. The most frequent location is between the third and fourth metatarsals (third webspace). Other, less common locations are between the second and third metatarsals (second webspace) and, rarely, between the first and second (first webspace) or fourth and fifth (fourth webspace) metatarsals.
Morton neuroma (interdigital neuroma), first described in 1876, is a perineural fibrosis and nerve degeneration of the common digital nerve. Morton neuroma, or Morton's neuroma, is not a true neuroma, although it results in neuropathic pain in the distribution of the interdigital nerve secondary to repetitive irritation of the nerve. The most frequent location is between the third and fourth metatarsals (third webspace). Other, less common locations are between the second and third metatarsals (second webspace) and, rarely, between the first and second (first webspace) or fourth and fifth (fourth webspace) metatarsals.
Causes
Pronation of the foot can cause the metatarsal heads to rotate slightly and pinch the nerve running between the metatarsal heads. This chronic pinching can make the nerve sheath enlarge. As it enlarges it than becomes more squeezed and increasingly troublesome. Tight shoes, shoes with little room for the forefoot, pointy toeboxes can all make this problem more painful. Walking barefoot may also be painful, since the foot may be functioning in an over-pronated position.
Symptoms
Patients with a Morton's neuroma typically experience a sharp, shooting or burning pain, usually at the base of the forefoot or toes, which radiates into the two affected toes. Sometimes the pain may also radiate into the foot. The pain is often associated with the presence of pins and needles and numbness.
Diagnosis
A thorough subjective and objective examination from a physiotherapist is usually sufficient to diagnose a Morton's neuroma. Investigations such as an X-ray, ultrasound, MRI, CT scan or bone scan may sometimes be used to assist with diagnosis, assess the severity of the injury and rule out other conditions.
Non Surgical Treatment
Common treatments involve wearing different shoes or using arch supports. Resting the foot, massaging the toes and using an ice pack may work for some people. A GP or a podiatrist (foot specialist) may also recommend anti-inflammatory painkillers or a course of steroid injections. Numbing injections, in which alcohol and a local anaesthetic are injected into the affected area of the foot, may also be effective. In extreme cases, when the condition does not respond to treatment, day case surgery may be needed.
Surgical Treatment
Surgery for Morton's neuroma is usually a treatment of last resort. It may be recommended if you have severe pain in your foot or if non-surgical treatments haven't worked. Surgery is usually carried out under local anaesthetic, on an outpatient basis, which means you won't need to stay in hospital overnight. The operation can take up to 30 minutes. The surgeon will make a small incision, either on the top of your foot or on the sole. They may try to increase the space around the nerve (nerve decompression) by removing some of the surrounding tissue, or they may remove the nerve completely (nerve resection). If the nerve is removed, the area between your toes may be permanently numb. After the procedure you'll need to wear a special protective shoe until the affected area has healed sufficiently to wear normal footwear. It can take up to four weeks to make a full recovery. Most people (about 75%) who have surgery to treat Morton's neuroma have positive results and their painful symptoms are relieved.
Morton neuroma (interdigital neuroma), first described in 1876, is a perineural fibrosis and nerve degeneration of the common digital nerve. Morton neuroma, or Morton's neuroma, is not a true neuroma, although it results in neuropathic pain in the distribution of the interdigital nerve secondary to repetitive irritation of the nerve. The most frequent location is between the third and fourth metatarsals (third webspace). Other, less common locations are between the second and third metatarsals (second webspace) and, rarely, between the first and second (first webspace) or fourth and fifth (fourth webspace) metatarsals.Causes
Pronation of the foot can cause the metatarsal heads to rotate slightly and pinch the nerve running between the metatarsal heads. This chronic pinching can make the nerve sheath enlarge. As it enlarges it than becomes more squeezed and increasingly troublesome. Tight shoes, shoes with little room for the forefoot, pointy toeboxes can all make this problem more painful. Walking barefoot may also be painful, since the foot may be functioning in an over-pronated position.
Symptoms
Patients with a Morton's neuroma typically experience a sharp, shooting or burning pain, usually at the base of the forefoot or toes, which radiates into the two affected toes. Sometimes the pain may also radiate into the foot. The pain is often associated with the presence of pins and needles and numbness.
Diagnosis
A thorough subjective and objective examination from a physiotherapist is usually sufficient to diagnose a Morton's neuroma. Investigations such as an X-ray, ultrasound, MRI, CT scan or bone scan may sometimes be used to assist with diagnosis, assess the severity of the injury and rule out other conditions.
Non Surgical Treatment
Common treatments involve wearing different shoes or using arch supports. Resting the foot, massaging the toes and using an ice pack may work for some people. A GP or a podiatrist (foot specialist) may also recommend anti-inflammatory painkillers or a course of steroid injections. Numbing injections, in which alcohol and a local anaesthetic are injected into the affected area of the foot, may also be effective. In extreme cases, when the condition does not respond to treatment, day case surgery may be needed.
Surgical Treatment
Surgery for Morton's neuroma is usually a treatment of last resort. It may be recommended if you have severe pain in your foot or if non-surgical treatments haven't worked. Surgery is usually carried out under local anaesthetic, on an outpatient basis, which means you won't need to stay in hospital overnight. The operation can take up to 30 minutes. The surgeon will make a small incision, either on the top of your foot or on the sole. They may try to increase the space around the nerve (nerve decompression) by removing some of the surrounding tissue, or they may remove the nerve completely (nerve resection). If the nerve is removed, the area between your toes may be permanently numb. After the procedure you'll need to wear a special protective shoe until the affected area has healed sufficiently to wear normal footwear. It can take up to four weeks to make a full recovery. Most people (about 75%) who have surgery to treat Morton's neuroma have positive results and their painful symptoms are relieved.
For Leg Length Discrepancy Podiatrists Prefer Shoe Lifts
There are two different types of leg length discrepancies, congenital and acquired. Congenital indicates that you are born with it. One leg is structurally shorter compared to the other. As a result of developmental stages of aging, the brain senses the stride pattern and identifies some variance. Our bodies usually adapts by tilting one shoulder over to the "short" side. A difference of under a quarter inch is not grossly abnormal, does not need Shoe Lifts to compensate and typically doesn't have a profound effect over a lifetime.

Leg length inequality goes largely undiscovered on a daily basis, however this issue is easily fixed, and can reduce a number of cases of back problems.
Therapy for leg length inequality usually involves Shoe Lifts. These are generally low-priced, regularly priced at below twenty dollars, in comparison to a custom orthotic of $200 plus. When the amount of leg length inequality begins to exceed half an inch, a whole sole lift is generally the better choice than a heel lift. This prevents the foot from being unnecessarily stressed in an abnormal position.
Low back pain is the most prevalent health problem affecting people today. Around 80 million men and women are afflicted by back pain at some stage in their life. It's a problem which costs businesses millions every year due to time lost and productivity. New and superior treatment methods are constantly sought after in the hope of reducing the economic impact this issue causes.

People from all corners of the earth experience foot ache due to leg length discrepancy. In most of these cases Shoe Lifts are usually of very beneficial. The lifts are capable of alleviating any pain in the feet. Shoe Lifts are recommended by countless certified orthopaedic practitioners".
In order to support the human body in a healthy and balanced manner, the feet have got a crucial job to play. In spite of that, it's often the most overlooked region in the human body. Some people have flat-feet which means there is unequal force placed on the feet. This will cause other body parts including knees, ankles and backs to be affected too. Shoe Lifts guarantee that ideal posture and balance are restored.
Leg length inequality goes largely undiscovered on a daily basis, however this issue is easily fixed, and can reduce a number of cases of back problems.
Therapy for leg length inequality usually involves Shoe Lifts. These are generally low-priced, regularly priced at below twenty dollars, in comparison to a custom orthotic of $200 plus. When the amount of leg length inequality begins to exceed half an inch, a whole sole lift is generally the better choice than a heel lift. This prevents the foot from being unnecessarily stressed in an abnormal position.
Low back pain is the most prevalent health problem affecting people today. Around 80 million men and women are afflicted by back pain at some stage in their life. It's a problem which costs businesses millions every year due to time lost and productivity. New and superior treatment methods are constantly sought after in the hope of reducing the economic impact this issue causes.
People from all corners of the earth experience foot ache due to leg length discrepancy. In most of these cases Shoe Lifts are usually of very beneficial. The lifts are capable of alleviating any pain in the feet. Shoe Lifts are recommended by countless certified orthopaedic practitioners".
In order to support the human body in a healthy and balanced manner, the feet have got a crucial job to play. In spite of that, it's often the most overlooked region in the human body. Some people have flat-feet which means there is unequal force placed on the feet. This will cause other body parts including knees, ankles and backs to be affected too. Shoe Lifts guarantee that ideal posture and balance are restored.
Learn How To Treat Posterior Calcaneal Spur

Overview
A heel spur is a projection or growth of bone where certain muscles and soft tissue structures of the foot attach to the bottom of the heel. Most commonly, the plantar fascia, a broad, ligament-like structure extending from the heel bone to the base of the toes becomes inflamed, and symptoms of heel pain begin. As this inflammation continues over a period of time, with or without treatment, a heel spur is likely to form. If heel pain is treated early, conservative therapy is often successful, and surgery is usually avoided.
Causes
One common cause of heel spurs and related injuries is due to abnormal mechanics and movement of the foot, also referred to as pronation. Abnormal gait, which is the way our feet hit the ground as we walk, also stresses the tissue of the foot, leading to conditions such as plantar fasciitis and heel spurs. Pronation can cause the foot to become unstable during movement, affecting the gait and leading to damage. A sudden increase in weight can also influence the development of a painful heel spur.

Symptoms
If your body has created calcium build-ups in an effort to support your plantar fascia ligament, each time you step down with your foot, the heel spur is being driven into the soft, fatty tissue which lines the bottom of your heel. Heel spur sufferers experience stabbing sensations because the hard protrusion is literally being jabbed into the heel pad. If left untreated, Plantar Fasciitis and heel spurs can erode the fatty pad of the heel and cause permanent damage to the foot. Fortunately, most cases can be resolved without medications or surgeries.
Diagnosis
Sharp pain localized to the heel may be all a doctor needs to understand in order to diagnose the presence of heel spurs. However, you may also be sent to a radiologist for X-rays to confirm the presence of heel spurs.
Non Surgical Treatment
If pain and other symptoms of inflammation-redness, swelling, heat-persist, you should limit normal daily activities and contact a doctor of podiatric medicine. The podiatric physician will examine the area and may perform diagnostic X-rays to rule out problems of the bone. Early treatment might involve oral or injectable anti-inflammatory medication, exercise and shoe recommendations, taping or strapping, or use of shoe inserts or orthotic devices. Taping or strapping supports the foot, placing stressed muscles and tendons in a physiologically restful state. Physical therapy may be used in conjunction with such treatments. A functional orthotic device may be prescribed for correcting biomechanical imbalance, controlling excessive pronation, and supporting of the ligaments and tendons attaching to the heel bone. It will effectively treat the majority of heel and arch pain without the need for surgery. Only a relatively few cases of heel pain require more advanced treatments or surgery. If surgery is necessary, it may involve the release of the plantar fascia, removal of a spur, removal of a bursa, or removal of a neuroma or other soft-tissue growth.
Surgical Treatment
When chronic heel pain fails to respond to conservative treatment, surgical treatment may be necessary. Heel surgery can provide pain relief and restore mobility. The type of procedure used is based on examination and usually consists of releasing the excessive tightness of the plantar fascia, called a plantar fascia release. The procedure may also include removal of heel spurs.
Prevention
Walk around before you buy shoes. Before you purchase your shoes, do the following. Re-lace the shoes if you're trying on athletic shoes. Start at the farthest eyelets and apply even pressure to the laces as you come closer to the tongue of the shoe. Make sure that you can wiggle your toes freely inside of the shoe. Also, make sure that you have at enough space between your tallest toe and the end of the shoe. You should have room equal to about the width of your thumb in the tip of your shoe. Walk around to make sure that the shoe has a firm grip on your heel without sliding up and down. Walk or run a few steps to make sure your shoes are comfortable. Shoes that fit properly require no break-in period.